Compatible Devices with Boston Cross Check
December 31, 2025
Cycle Charting After Hysterectomy
I often get asked whether cycle charting is possible following a hysterectomy (surgical removal of the uterus) and I think it's a great question because the answer isn't super straightforward all the time. The intuition is: "if I still have my ovaries, then I'm still ovulating.... and so I could chart that, right? But.... how?????"
So let's begin by talking about types of hysterectomies, because that will be important for understanding what you could be able to track (and how!):
- Total hysterectomy= removal of the uterus and cervix. Ovaries remain intact.
- Supracervical hysterectomy (also called partial or subtotal)= removal of the main part of the uterus, but leaves the cervix intact.
- Hysterectomy with Oophorectomy= removal of the uterus and one or both of the ovaries, sometimes including the fallopian tubes (so you can think of this one as having multiple sub-types as well).
- Radical Hysterectomy= removal of the uterus and cervix, tissue surrounding the cervix, the top part of the vaginal canal, and sometimes the pelvic lymph nodes.
The most common type is a total hysterectomy, so we'll start by talking about charting in that particular case.
Charting in the Most Typical Case Post-Hysterectomy
If a woman has had a total hysterectomy, then charting is complicated by the absence of a couple of key biomarkers: bleeding (periods!) and cervical fluid.* The uterus is no longer there to build up endometrial lining and the cervix is no longer there to create cervical fluid (or: cervical mucus). So especially if you've been using an ovulation method like Billings or Creighton which relies exclusively on these biomarkers, you might be wondering whether there's anything left to track!
The "secret" lies in remembering that all those handy terms we commonly use to describe the phases of the menstrual cycle are actually terms for the ovarian cycle.
- The follicular phase describes the period of time prior to ovulation when the egg is developing within a follicle in the ovary.
- The luteal phase describes the period of time after ovulation when the follicle has undergone luteinization and has become the corpus luteum.
So it's definitely possible to speak of (and think of!) a full menstrual cycle with reference to just the ovaries, not the uterus.
(Fun trivia fact: the uterine cycle consists of the menstrual phase during a period, the proliferative phase when lining is being built up, and the secretory phase when glands in the uterine lining are releasing key nutrients to prepare for implantation)
With that in mind, we can now think about which key hormones are still functioning and how to track them:
- FSH is still being sent from the pituitary gland, to signal follicular development
- Estrogen is still being produced in the ovary as the follicle matures
- LH is still being sent from the pituitary gland to ripen the follicle and open it for ovulation
- Progesterone is still being produced by the corpus luteum in the ovary after ovulation
Therefore, with current at-home monitoring techniques, the following standard NFP biomarkers could be observed:
- Estrogen, LH, and progesterone can be observed through urinary metabolites either with a monitor that tracks multiple hormones or with stand-alone LH tests (aka OPKs) or with PdG (progesterone) tests
- Progesterone effects can be tracked through observing shifts in basal body temperature (BBT)
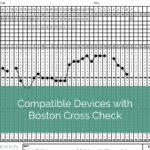
Within the Boston Cross Check system (the NFP method that I teach), the standard option for tracking cycles following a total hysterectomy would be to use the Clearblue Monitor + BBT, yielding a chart that looks something like this:
|
|
I've modified one of my personal BCC charts to only show Monitor + Temps, so this is not an actual case study, but here's what I want to show you: even though there is no bleeding or cervical fluid, the ability to still find a monitor peak reading and a temperature shift allows us to calculate both the start and the end of fertility for this particular cycle, even without additional biomarkers.
But without the bleeding, how can we know which day is Cycle Day 1?
Well, that's a good question. And that's why I would highly recommend tracking with BBT instead of relying on either PdG (urinary metabolite) testing or even a family planning blood draw to track progesterone activity in this case. If you are confirming ovulation with a blood test, that's just one data point on one day. It tells you whether you've ovulated, but doesn't tell you anything about progesterone patterns beyond that. A similar thing happens with PdG testing: maybe you can get a few days' worth of data to help show a progesterone arc that confirms ovulation, but the cost of testing every day is probably going to be prohibitive and would also require some additional skill at observing your personal baseline levels to know whether you can see a quantitative drop that signals the likely onset of a period.
However, with consistent temperature tracking, we already have an established set of research and calculations that will allow you to have a pretty good idea of when your hormones are shifting to signal the start of a new cycle. Note on the chart above that there is a temperature dip down below the coverline on Cycle Day 27. While not a universal marker, many women do see a temperature drop either right before or right at the start of their period. It's not a perfect system when you don't have the bleeding sign to compare to the temperature sign, but in many cases it gives you a fair idea of the timing of hormonal activity. And if you work with an instructor, they can advise on more specifics about managing charts like this within your chosen charting system— even if you don't quite meet this pattern and tend to have temps that remain elevated during the first few days of a new cycle.
So which systems could be considered for charting in this situation?
- The Marquette Model will offer standard options for Clearblue and Mira monitor (altho keep in mind that Mira protocols are still in the experimental or "soft protocol" stages) plus optional BBT.
- Boston Cross Check offers Clearblue and BBT as a standard protocol option for all users. Temperature-only tracking could also be utilized with alternate calculation rules. In the latter situation, you lack an estrogenic biomarker because you are essentially just tracking progesterone activity, but this is compensated for by algorithmic calculations based on previous temps shifts or could be moot if you only wanted to use post-ovulatory days for intercourse anyway. BBT + LH testing could also be utilized with the same restrictions.
- FEMM includes LH tracking, and some instructors are also able to incorporate temperatures if needed, altho it's not a standard part of their protocols. The tricky part in this situation is that you are lacking any estrogenic tracking since you're using OPKs instead of a combined hormone monitor, but same comments apply as above.
- Sympto-Thermal Methods like SymptoPro or Couple to Couple League will have alternate protocols for tracking temperature-only in the absence of cervical fluid, with various modifications to consider according to couple preference and situation. Again: in this situation you lack an estrogenic biomarker so the same comments apply as above.
Taking this knowledge, we can then see how cycle tracking following another type of hysterectomy may or may not be affected:
- Following a supracervical hysterectomy, there is no uterus (therefore no bleeds) but it's possible that the cervical crypts may still respond to estrogen production in the ovaries and therefore cervical fluid could be added to the tracking system.
- Following a hysterectomy with oophorectomy, you'll either have no ovaries (in which case: no cycle at all which means nothing to track) or you'll have just one ovary, which still may allow you to track with the options noted above.
- Following a radical hysterectomy, it's still possible the ovaries are intact despite all of the other removals... and so tracking with the above options could still be possible.
Now, let's add one extra little wrench into the conversation which is the fact that regardless of when you had your hysterectomy, if you still have your ovaries you will go through the stages of perimenopause— a transition which can last many years and will come with many cycle changes!
Perimenopause changes can pose a challenge even when a woman still has her uterus, which is why I'll strongly suggest again that working with a certified instructor in a proven method of NFP can be absolutely crucial for helping you figure this out! At some point, LH disturbances combined with estrogen and progesterone deficiencies can complicate tracking with urinary metabolites and BBT, so an instructor can help you talk through various options, adapt protocols in light of these expected challenges, and offer a line of direct support as you navigate the natural changes that come with perimenopause.
But wait: why would charting even be important?
Given that charting following a hysterectomy can be complicated and may even require totally changing your charting method, it's worth asking whether going through all this rigmarole is even worth it! Fair question.
The reasons for charting following a hysterectomy boil down to personal preference and utility, but fall into two categories: for the monitoring of general reproductive health (including tracking of perimenopausal changes) and to avoid the possibility of an ectopic pregnancy.
If a woman is still ovulating and lacks a uterus, traditional pregnancy with implantation in the uterine wall is not possible. However, there is a very small chance still that an embryo could implant in a different location and result in an ectopic pregnancy, which would be very serious. By charting your cycle, couples can still avoid intercourse on potentially fertile days to significantly minimize this risk.
Conclusion
In summary, cycle charting following a hysterectomy will vary depending on the type of hysterectomy and the preferences of the couple. Despite posing some notable challenges, in many cases it is still possible to observe and chart ovarian function even without some key biomarkers— but having an experienced NFP instructor to guide you through the process and help you make adjustments can be an invaluable help!
----
*It's important to remember that there are vaginal secretions other than cervical fluid which may still be observable. For example: the Bartholin's and Skene's glands can still produce lubrication around sexual arousal, and discharge can still be noticed in the presence of a yeast infection, bacterial vaginosis, or any other vaginal infection. However, none of these would be charted as biomarkers for ovulation.
 Loved this post? Be sure to subscribe to the Body Lit Library weekly newsletter, where every Thursday you'll get access to new content, updates, and special insider offers!
Loved this post? Be sure to subscribe to the Body Lit Library weekly newsletter, where every Thursday you'll get access to new content, updates, and special insider offers!
 Want to learn more? Check out our lifelong body literacy education courses and books, from puberty through perimenopause and everything in between: pearlandthistle.com
Want to learn more? Check out our lifelong body literacy education courses and books, from puberty through perimenopause and everything in between: pearlandthistle.com